
Across the NHS, infection prevention teams, operational managers, and procurement leads are facing an increasingly difficult balancing act: how do you safely isolate infectious patients when side rooms are limited, wards are full, and pressures continue year-round?
Respiratory infections remain one of the biggest operational and clinical challenges for UK hospitals. Seasonal influenza, COVID-19, RSV, norovirus, tuberculosis, and other airborne pathogens continue to place significant strain on acute care settings, particularly in emergency departments, assessment units, and high-occupancy wards.
At the same time, hospitals are under unprecedented bed pressure.
Recent NHS reporting has highlighted ongoing overcrowding and capacity issues across UK hospitals, with rising emergency admissions and increased winter escalation events. The challenge is no longer simply treating infectious patients quickly, it is finding safe, practical ways to isolate them without compromising bed availability or operational flow.
This is where CLS Surgical and the ShareGuard99 patient isolation system provide a highly effective, cost efficient and clinically relevant solution.
The growing challenge of isolation capacity in NHS hospitals
The importance of rapid patient isolation is well established within infection prevention and control (IPC) guidance. However, the reality across many NHS sites is that there simply are not enough single rooms available.
The Royal College of Emergency Medicine’s (RCEM) national Infection Prevention and Control report found that isolation performance in UK emergency departments has deteriorated significantly, with delays to isolating vulnerable or infectious patients increasing nationally.
The same report showed:
- National average time to isolate vulnerable patients increased to over 134 minutes
- Only around 19% of identified vulnerable patients were moved to a side room
- Screening and infection control performance has declined across multiple IPC measures
UKHSA’s latest healthcare-associated infection survey also reported that healthcare-associated infections (HCAIs) were present in 7.6% of patients across England, an increase compared with previous reporting periods.

Meanwhile, frontline clinicians continue to report severe operational limitations caused by outdated hospital infrastructure and insufficient isolation facilities. In a recent interview discussing winter pressures, an NHS emergency medicine consultant stated:
“We don’t have enough single rooms to actually isolate patients in.”
For IPC teams, this creates a difficult operational reality:
- Infectious patients often remain in shared clinical spaces
- Side rooms must be prioritised for only the highest-risk patients
- Bed flow slows due to isolation bottlenecks
- Staff exposure risks increase, which could leave to further issues due to staff shortages from illness
- Ward outbreaks become more likely
- Elective activity and capacity management are affected
The problem is no longer hypothetical, it is operational, daily, and financially significant. Many hospital wards throughout the UK, particularly in older hospitals, are dated with old architecture that doesn’t facilitate a lot of single rooms. As ‘corridor care’ becomes the norm in more hospitals, when patients come in with respiratory infections, it makes it far more challenging to effectively maintain infection control.
Why traditional isolation models are no longer enough
Historically, hospitals have relied on:
- Dedicated isolation rooms
- Cohorting patients
- Ward closures
- Temporary escalation spaces
However, these approaches all carry limitations. Building additional side rooms is expensive, time-consuming, and often impossible within older NHS estates. Cohorting can only be used safely when infections are confirmed and compatible. Ward closures create substantial operational disruption and lost capacity.
Modern infection prevention strategies now require solutions that are rapidly deployable, flexible across different wards and departments, cost-effective and compatible within the existing hospital infrastructure. This is precisely why ShareGuard99 is the ideal solution for infection control and prevention.

ShareGuard99: Isolation at the bedside
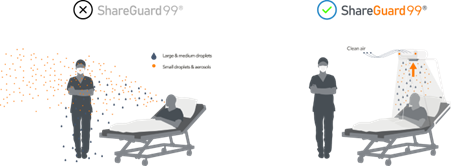
The ShareGuard99 allows hospitals to create an isolated patient environment directly at the bedside without requiring a dedicated side room. Featuring a specially designed air purifying unit which attaches directly to a patient’s bed, with a single-use hood attached that covers the patient to create their own isolated space.
This innovative design traps aerosols and droplets generated by the infected patients and purifies the air for them. It is fully compatible with other care equipment, such as oxygen therapy and patient monitoring devices, too.
Designed specifically for healthcare settings, ShareGuard99 helps contain respiratory pathogens around the patient while maintaining visibility, accessibility, and workflow efficiency for clinical staff.
For hospitals struggling with:
- Respiratory infection surges
- Limited isolation rooms
- Emergency department overcrowding
- Seasonal escalation pressures
- Mixed acuity ward management
ShareGuard99 offers a practical and scalable infection control solution. Quick, compact and easy to use the ShareGuard99 in an incredibly cost-effective solution to tackle a number of issues hospitals face.

Key benefits for infection prevention and operational teams
Enhanced infection control
By isolating potentially infectious respiratory patients at the bedside, ShareGuard99 helps reduce the risk of airborne transmission to:
- Other patients
- Clinical staff
- Visitors
- Shared ward environments
This supports broader IPC objectives and can help reduce the likelihood of healthcare-associated outbreaks.
Increased bed capacity utilisation
One of the biggest operational advantages is the ability to continue safely using shared clinical areas when side rooms are unavailable.
Rather than leaving patients waiting in emergency departments, corridors, temporary escalation areas or assessment units, hospitals can create protected isolation spaces rapidly and efficiently. This helps maintain patient flow while supporting safer care delivery.
Cost-effective alternative to infrastructure expansion
Creating additional permanent isolation rooms requires:
- Major capital investment
- Estates work
- Ventilation modifications
- Significant operational disruption
ShareGuard99 provides a far more cost-effective alternative by transforming existing bed spaces into isolation-capable environments.
For procurement and operational teams, this represents:
- Lower upfront costs
- Faster deployment
- Better flexibility
- Reduced infrastructure dependency
Rapid deployment during winter pressures and outbreaks
Respiratory surges rarely arrive with warning. Hospitals need solutions that can be deployed immediately during:
- Flu season
- COVID surges
- RSV spikes
- Norovirus outbreaks
- High-demand winter periods
ShareGuard99 enables hospitals to expand isolation capability quickly without waiting for physical bed reconfiguration or ward redesign.
Improved staff confidence and safety
Protecting healthcare workers remains a critical priority. Especially in busy periods like flu season where increased capacity coupled staff shortages can lead to huge issues. Solutions that visibly support infection containment can help:
- Improve staff confidence
- Reduce anxiety around exposure
- Support safer clinical workflows
- Reinforce IPC compliance
- Minimise shortages in the busiest periods
In high-pressure environments, practical and visible infection control measures matter.
Ease of use and low maintenance
The ShareGuard99 is incredibly simple to use, the frame is installed onto a standard hospital bed, attach the hood to the air purifying unit and cover the patient with it, and then switch on the machine. It can then be used to isolate the patient for as long as needed, while still allowing for accessibility for treatments and other care equipment, and allowing the patient full visibility outside the cover.
After use, simply remove and dispose of the hood and clean the machine. While the hoods are single use, the filter on the ShareGuard99 only needs changing once every 6 months. This allows for 6 months

Supporting NHS priorities around patient safety and flow
The NHS continues to face sustained pressure from delayed discharges, emergency admissions, ageing infrastructure, and increasing respiratory demand. At the same time, infection prevention standards remain non-negotiable.
Hospitals therefore need solutions that bridge both priorities:
- Maintaining patient flow
- Improving infection containment
ShareGuard99 directly addresses both challenges.
It enables hospitals to:
- Isolate infectious patients more effectively
- Reduce reliance on scarce side rooms
- Maintain operational flexibility
- Improve resilience during surge events
- Support safer ward management
Importantly, it does this without requiring major infrastructure changes, representing the most cost-effective option for hospitals.

A smarter approach to modern hospital isolation
The reality for many NHS trusts is that side-room availability alone can no longer meet demand.
As healthcare-associated infections rise and hospitals continue to experience capacity pressures, innovative bedside isolation solutions like the ShareGuard99 are becoming increasingly important within modern IPC strategies.
CLS Surgical has positioned the ShareGuard99 as a practical, scalable, and cost-effective solution for healthcare providers needing to improve respiratory isolation capability without compromising bed capacity.
For infection prevention leads, operational managers, procurement teams, and hospital decision-makers, ShareGuard99 represents an opportunity to strengthen both patient safety and operational resilience.
Learn more about ShareGuard99
To learn more about how ShareGuard99 can support your hospital’s infection prevention and capacity management strategy, contact CLS Surgical to discuss deployment options, product specifications, and implementation support. Email us at customerservice@clssurgical.com, call us, 0151 733 1900, or fill in our online enquiry form.